















More than two years after a federal hospital price transparency rule took effect, PatientRightsAdvocate.org finds that only 24.5% of 2,000 hospitals examined nationwide are fully complying with every aspect of it. This conclusion is in line with other studies, including a January Journal of General Internal Medicine report that found a 35.9% compliance rate as of late 2022.
In contrast, a recent Centers for Medicare and Medicaid Services analysis of 600 hospitals claims 70% are following the rule. The American Hospital Association is championing this finding to suggest its members are complying with the rule.
However, CMS’s analysis that produced this over-optimistic compliance finding is insufficient. CMS’s hospital website review reveals no specific hospital transparency data or even the names of the hospitals analyzed. It only provides a surface-level look at compliance and does not analyze the price disclosures themselves for completeness of discounted cash prices and all insurance plan rates, as the rule requires.
CMS’s study even admits it “does not include all the requirements of the Hospital Price Transparency regulation” and “is not intended to be used to assess a hospital’s compliance.”
Yet AHA erroneously draws on the CMS finding to claim its member hospitals have made “a huge step forward” in complying with the rule. If that were true, American healthcare consumers would be able to search online for upfront hospital prices by now and spot the vast price differences for the same care. We’d be able to hold hospitals accountable for overcharging, have easy recourse in the case of overbilling, and enjoy substantial healthcare savings.
A recent NBC Nightly News segment on the hospital price transparency rule provides more detail on the disconnect between these studies’ findings. Presented with proof by NBC that hospitals often put “N/A” values in place of actual prices in their disclosure files, CMS administrator Chiquita Brooks-LaSure said the agency considers such hospitals compliant because N/As indicate hospitals don’t offer the associated procedures.
This explanation doesn’t hold water. Many hospitals nationwide post price files where the bulk of procedures feature N/As instead of prices. For instance, Maimonides Midwood Community Hospital in Brooklyn, NY, posts N/A for 98% of its insurance plan rates, and Ascension Genesys Hospital in Grand Blanc, MI, uses N/As for 92% of its rates. Mount Carmel East Hospital in Columbus, OH, puts N/As for 97% of its rates, and Holy Cross Hospital in Fort Lauderdale, FL, publishes N/As for 99%.
Are healthcare consumers really supposed to believe that these major American hospitals don’t offer any of these basic procedures where N/As are listed?
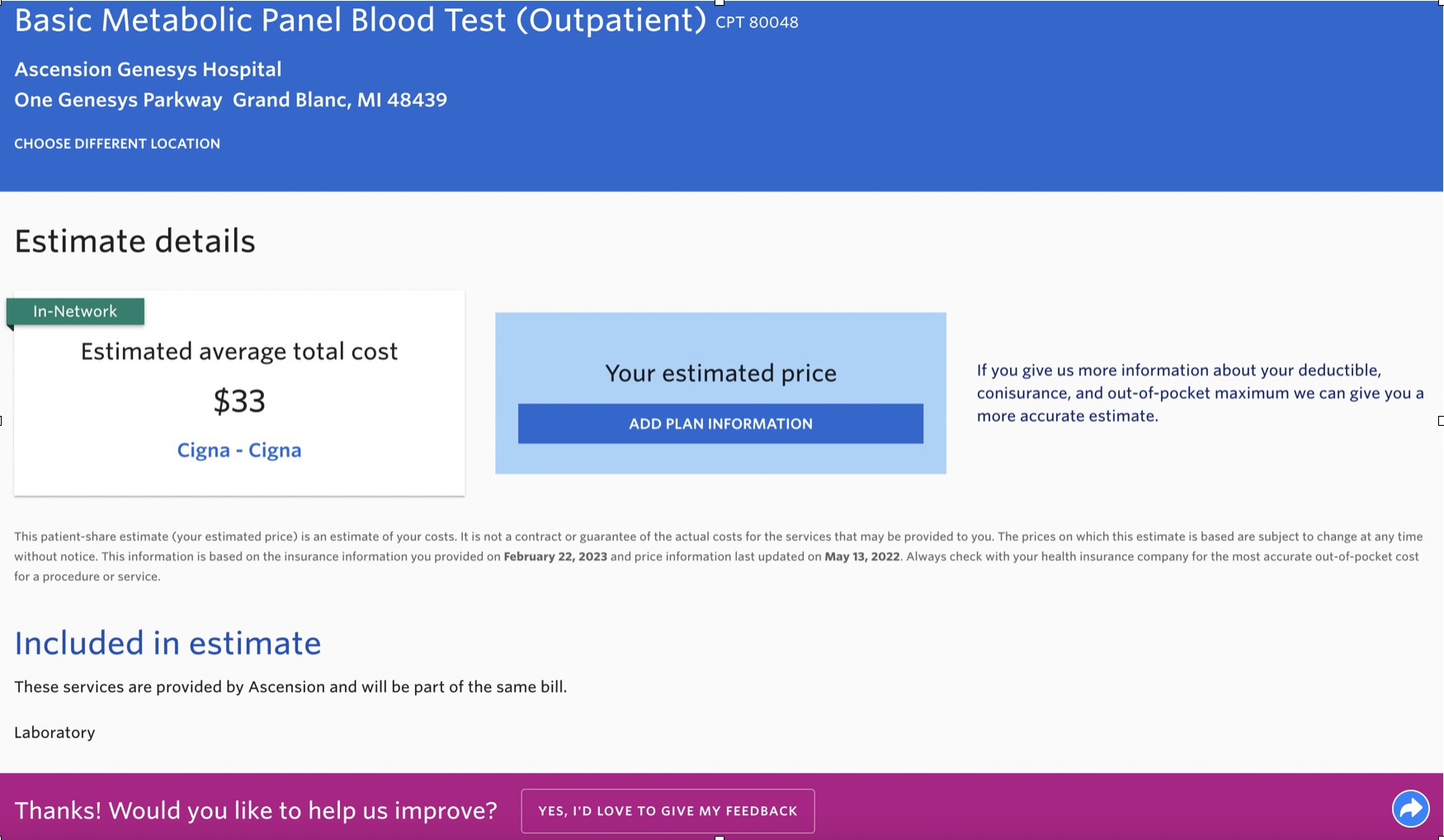
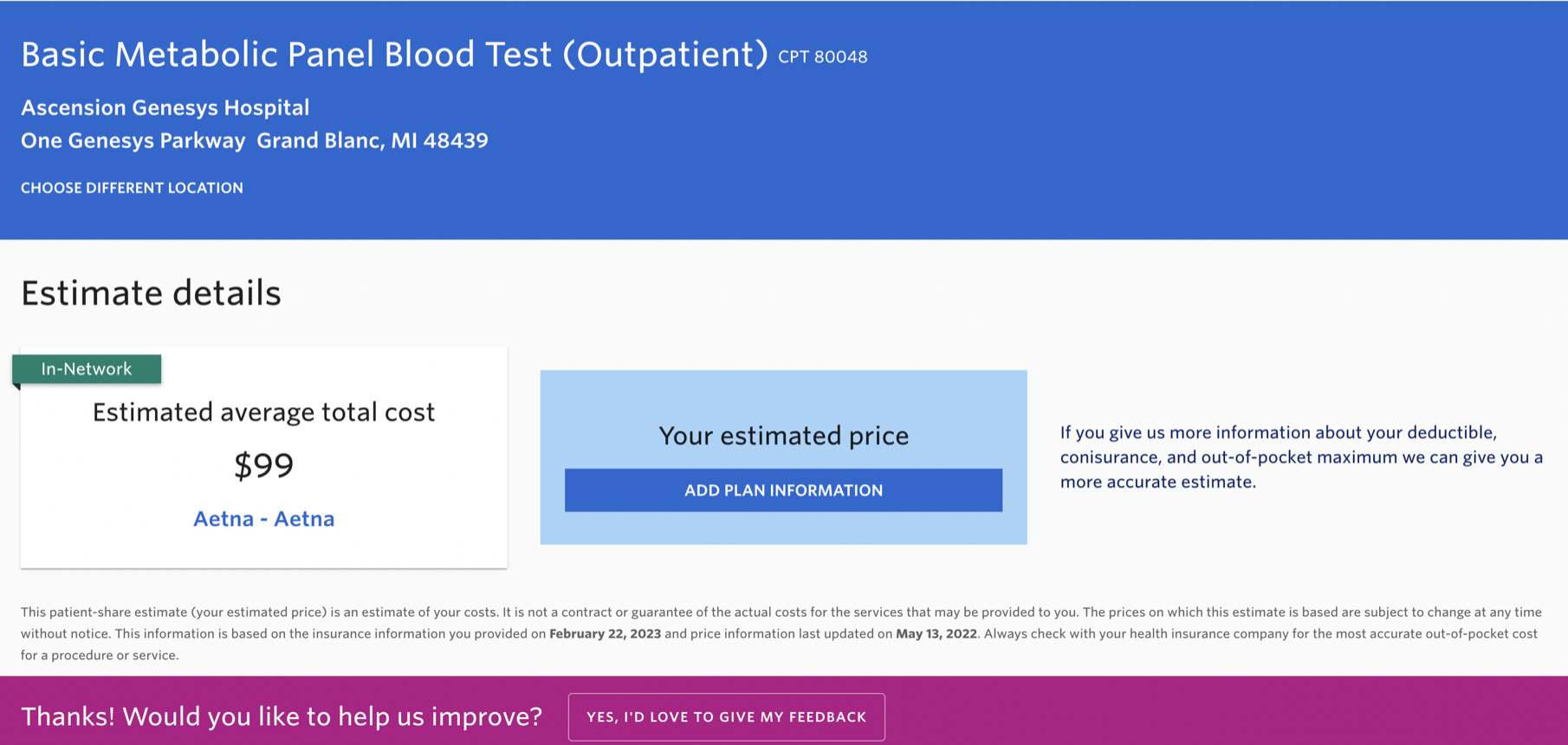
Further, hospitals’ N/A procedures routinely show up in hospitals’ price estimator tools, revealing hospitals do, in fact, offer them. For instance, Ascension Genesys lists N/A instead of Cigna and Aetna rates for a basic metabolic panel. Yet the hospital’s price estimator predicts this procedure costs $33 for Cigna patients and $99 for Aetna patients.
(Reminder: price estimates are no substitute for actual, upfront prices because they don’t hold hospitals accountable for dramatically higher final bills, and they prevent consumers from meaningful comparison shopping.)
Finally, hospitals’ N/A procedures routinely show up in health insurers’ price disclosures required by a separate health insurance price transparency mandate called the Transparency in Coverage rule. For instance, Maimonides Midwood Community Hospital lists N/As instead of Cigna prices for MRIs, CT scans, and mammograms. Yet Cigna’s Transparency in Coverage price file shows actual prices for these procedures at this hospital, proving they are indeed offered there.
This evidence suggests hospitals are exploiting the N/A loophole to continue hiding their actual prices from patients. At the very least, CMS should eliminate this hospital price transparency escape hatch and deem hospitals that mask real prices with N/As as noncompliant, in-line with PRA’s study methodology. Doing so would make CMS’ sunny compliance conclusion plummet.
Even by the results of its own analysis, CMS has inadequately enforced the price transparency rule. It has only fined two hospitals out of the approximately 1,800 it finds aren’t compliant. Yet even this meager response shows the value of robust enforcement. These two hospitals quickly became compliant and, to date, publish exemplary price files.
As a first step to move toward greater hospital price transparency and lower costs, CMS can immediately issue $2 million fines on the 30% of American hospitals it concludes are noncompliant. If CMS takes enforcement seriously, the hospital industry will respond by quickly coming into compliance.
After those hospitals post their actual prices, the agency can do another sweep of hospital price disclosures using a broader compliance criteria to identify another tranche that isn’t following all facets of the rule, such as posting N/As instead of complete and clear prices by insurance company and plan.
Such robust enforcement can usher in systemwide hospital price transparency required to empower patients, employers, and unions to shop for the best care at the best prices and fight medical billing overcharges, errors, and fraud. Pretending the widespread hospital noncompliance problem doesn’t exist only delays this pro-consumer healthcare revolution.
Photo: sinemaslow, Getty Images
Promoted

Payer’s Place: Dawn Maroney
Dawn Maroney, President, Markets of Alignment Health and CEO of Alignment Health Plan, to discuss how they are using technology to provide better service and care to consumers.
Promoted
![]()
Discover the Next-Gen Platform for Integrated Collaborative Care
Beyond EHRs and digital front doors, reducing the gaps in patient care journeys.



{kind=link}
{kind=link}